Accompanying symptoms of fever, their examination and significance
At the beginning of an illness we can notice various symptoms, even before fever:
- fussiness
- apathy, fatigue, drowsiness
- cuddly (need for proximity)
- loss of appetite
- shiny eyes
- lack of vigilance, lethargy
These symptoms typically change during different stages of the fever.
Symptoms accompanying fever
During the first phase of the fever at the ascent:
- paleness, marbly skin
- cold limbs and forehead,
- shivering, trembling, muscle trembling, small spasms during sleep
- general discomfort, fussiness, lethargy
During the second phase of the fever peak:
- flushing, red hot cheeks
- hot limbs
- drowsiness
- hallucinations due to fever
In the third phase of the fever at the beginning of the decrease:
- sweating, wet palms and foot soles
- thirst
During the fourth stage of fever, when body heat returns to normal:
- increasing activity
- returning appetite
Heart rate changes in optimal fever
The pulse can best be felt on the inside of the wrist in the shallow hollow below the base of the thumb (in case of infants and young children in the elbow on the inside of the upper arm). We place the tip of the first two (or three) fingers over the hollow, and hold the child’s wrist with our thumb from the opposite side. We count the heartbeat for 15 seconds. Multiplying the result by four we get the heartbeat per minute.
Normal range of heart rate for children at 10 min rest without fever:
|
Age |
Heart rate |
|
New-born |
100 - 180 / min |
|
1 - 11 months |
90 - 160 / min |
|
1 - 2 years |
85 - 150 / min |
|
3 - 4 years |
80 - 140 / min |
|
5 - 6 years |
75 - 120 / min |
|
7 - 9 years |
70 - 110 / min |
|
Above 10 years |
60 - 100 / min |
These rates might rise 5-25% in case of fever. This depends on age, weight, cause of fever, etc.
The algorhithm we have included in the application takes these factors into consideration.
In this case use the app.
Respiratory rate
In case of fever, breathing will increase with the heart rate.
For measuring respiratory rate: it is visible, audible, perceptible.
It can be seen in the movement of the chest and abdomen (possibly the wings of the nose).
It can be heard at the nostrils.
It is felt when our palms are placed on the abdomen or chest.
- the breathing rate is below or above the range in rest over more than 10 minutes,
- wheezing, whistling, forced breathing and bluish lips and skin at any age.
In case of fever, breathing will increase with the heart rate.
Normal range of breathing rate for a non-feverish child at 10 min of rest:
|
Age |
Respiratory rate |
|
0 - 1 year |
30 - 50 / min |
|
1 - 3 years |
24 - 40 / min |
|
3 - 6 years |
22 - 34 / min |
|
6 - 12 years |
18 - 30 / min |
|
Above 12 years |
12 - 20 / min |
These rates might rise 5-25% in case of fever. This depends on age, weight, cause of fever, etc.
The algorhithm we have included in the application takes these factors into consideration.
In this case use the app.
Immediate medical care needs to be sought if there is wheezing, whistling, forced breathing and bluish lips and skin at any age.
Pain
Head and limb pains typically occur with the influenza during the ascending phase of the fever.
A pain scale can be used to assess its severity.
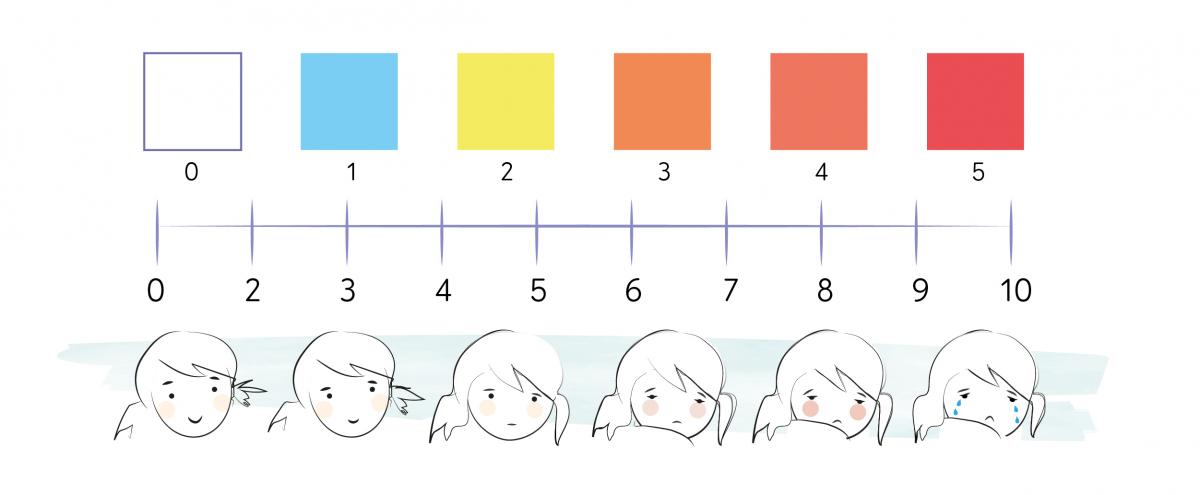
Diffuse general pain throughout the body is frequent and harmless. Muscles and joints are affected.
Limb pain deserves special attention if it is associated with localized (small site), worsening and possibly localized swelling. In this case, seek medical advice.
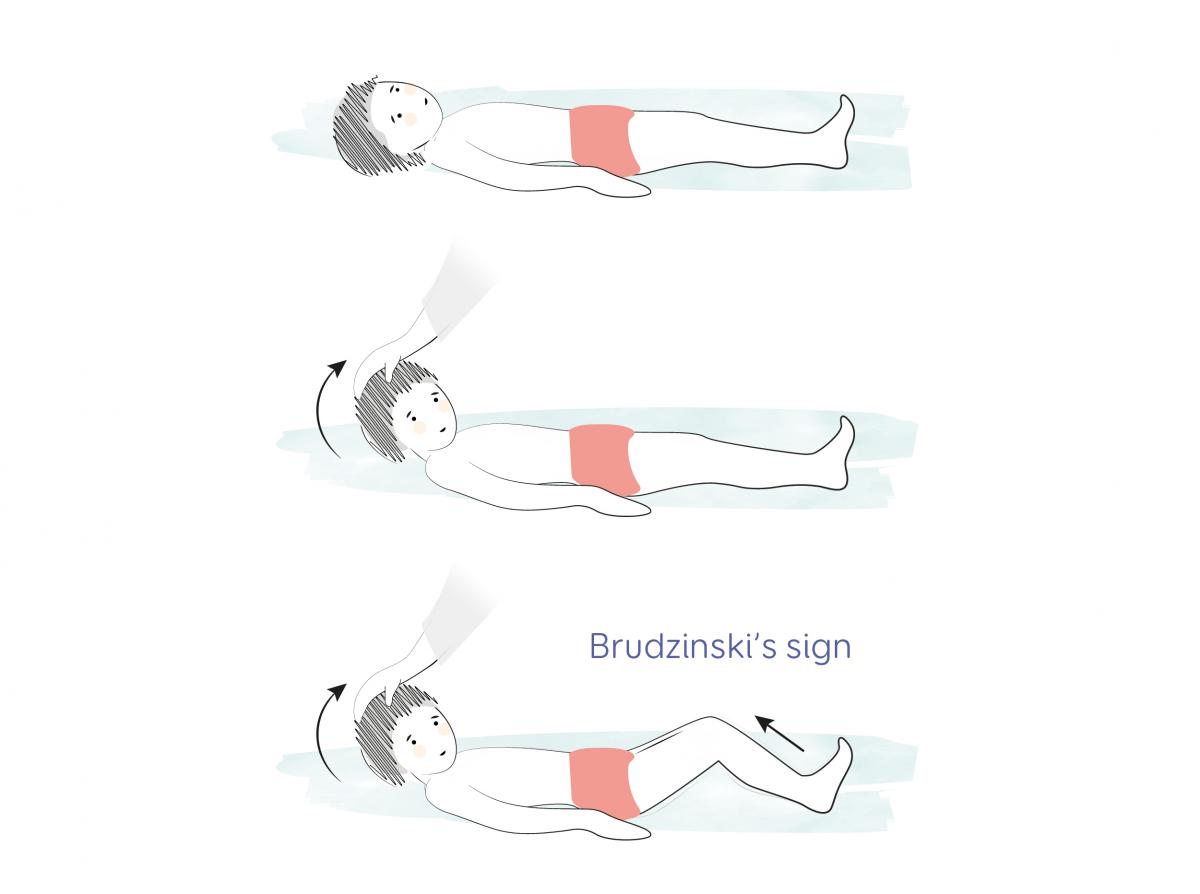
When fever elevates, headache is common.
If it’s accompanied by stiff neck, it may be a sign of meningitis. This can be demonstrated if when raising the head of the child lying on his back the child’s knees will also flex (Brudzinski’s sign).
Vomiting and diarrhoea
If both vomiting and diarrhea occur with fever, it can be a sign of common gastrointestinal infection.
Vomiting by itself can also be the sign of sunstroke, appendicitis, or rarely meningitis.
In a mild case have the child rest, make him drink water by sips, at small intervals. See more in the chapter „Care interventions during fever”.
Seek medical attention if:
- diarrhoea is bloody or has been going on for 12 hours continuously and/or
- vomiting for more than five hours, the vomit is frequent, biliary yellow and/or
- with severe stomach ache and/or a state of drowsiness.
Otherwise, rest and swallow liquid by single gulps at intervals.
Loss of appetite
Physiological loss of appetite is normal in a febrile state.
Nutrition should be a light diet by bites, as much as the child requires. Rice, millet, steamed vegetables cut into small bites, fruits. Preferably in the morning when the fever is lower.
Fluid loss and drinking
In case of infants and young children dehydration may develop more easily during a febrile illness.
The following can play a role in it:
- insufficient drinking
- sweating
- vomiting
- diarrhoea
If they occur at the same time, small children can dehydrate quickly.
Serious signs of dehydration that require medical help:

- Decreased urine volume. If a child does not pee for more than 12 hours, consult a physician.
- The turgor and firmness of the skin is reduced. A sign of this is that when the skin is lifted into the fold of the abdomen, it disappears much more slowly than normal, or not at all.
- When crying, the tearing decreases or stops. If no tears appear at all when crying, that needs to be taken seriously.
- Arched, deep-set eyes, not only rings under the eyes.
- In infants (up to 1.5 years of age), the large fontanelle is sunken. See the picture.
- Lethargy, intoxicated state of mind, in severe cases the child cannot be awakened or only briefly.
Important questions summarized:
- How much did he/she drink? If the child has not taken any sips for more than 12 hours, consult a doctor.
- When did the child urinate last? If he/she hasn’t urinated for more than 12 hours, see a doctor.
- Did the child have diarrhoea? Seek medical attention in the case of more than 12 hours of continuous or bloody stool.
- Was the child vomiting? If the womiting contains bile or blood and is frequent for more than five hours, seek medical help.
In case if minor symptoms (e.g. dry tongue) it is not necessary to see a doctor, but rehydration is important. See below.
Forms of rehydration:
-
Breastfeeding is best for breastfed babies. If the child pukes or vomits, you can try a small amount again after a 5-10 min break.
-
All liquids except cow's milk are suitable (but preferably not sugary and carbonated).
-
If accompanied by vomiting, diarrhoea, then we can give oral rehydration solution (ORS). When cool, the flavour can be tasted less. If the child will not drink it from a glass in sips, you can try a straw, a spoon or syringe, a few millilitres at a time. The ORS has the necessary amount of minerals (sodium, potassium, chlorine, citrate) and sugar (glucose).
-
See for more information the chapter „Care interventions during fever”.
Rash
Rashes may occur before, during or after fever.
Often before fever, it is a sign of infection at the end of the incubation period.
During fever it is often a sign of viral disease.
Rashes that occur after the fever has subsided are usually signs of a harmless viral infection, no action needs to be taken, no need to see a doctor.
These harmless rashes should be distinguished from dangerous purpuric rashes (petechiae) that require immediate medical attention.
Fortunately, the latter is very rare and easily distinguishable from harmless rash.
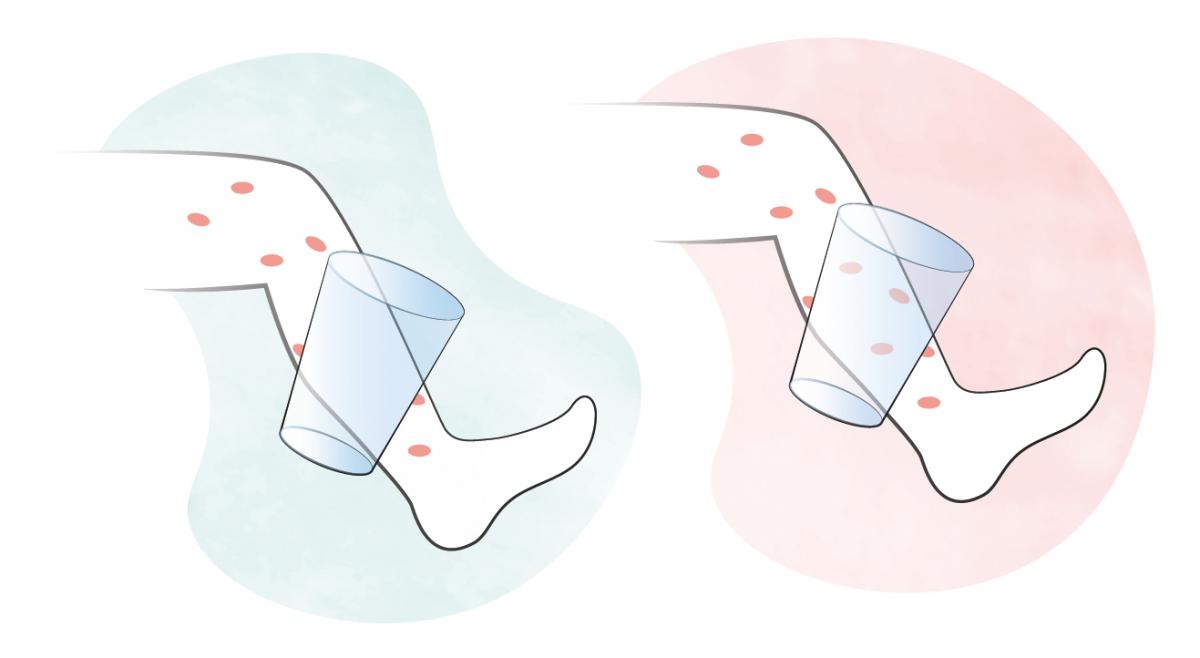
The glass test is suitable for this. Use a pair of glasses or a plain glass/plastic.
When applied to the skin, if the rash does not disappear it is purpuric rash. If it's gone, it's harmless (see the picture).
The rash on the left is not dangerous because it can be suppressed (blanching).
The red rash on the right is purpuric (non-blanching) rash and it's dangerous.
However, glass test should be repeated for every rash after 4-6 hours to see if it remains harmless.
You can find the corresponding numbered references here: References
Version update: 1 March 2024